






Testing for COVID-19
- Students vs. Pandemics
- May 18, 2020
- 6 min read
Updated: Nov 20, 2021
By Trang Truong

By now, a number of different methods have been developed to test for COVID-19 with many unique names for the same tests. This blog post will explain the basic scientific principles behind the most prominent COVID-19 assays. These screening methods typically fall into one of two categories: antigen assays or antibody assays.
Antigen Testing
Antigens are molecules that are capable of stimulating an immune response in the body. They are often present on the outside of pathogens, taking on many forms including proteins, peptides (chains of amino acids), sugars, and lipids. Different antigens are recognized by distinct antibodies (also known as immunoglobulins (Ig)) that bind to the antigens’ specific epitopes (surface features), eliciting certain immune responses. Exploiting this scientific principle, researchers have designed tests that detect antigens specific to the COVID-19 virus in order to determine who is infected by the disease. This type of testing is sometimes referred to as a diagnostic test or a viral test (1).
Antibody Testing
One of the primary ways that our body responds to infections is through the generation of antibodies. These antibodies bind to the antigens on pathogens so that our other immune cells (macrophages, dendritic cells, etc.) can better fight the infection. These antibodies can then continue circulating the body to combat future infections (2). Therefore, antibody tests (also called serologic tests) can tell us whether a person has been previously infected with COVID-19. However, antibody tests are not to be used to diagnose someone to be currently infected with COVID-19 since antibodies are made in the body 1-3 weeks after infection (3). Antibody tests have been refined to detect specific types of antibodies as well, allowing clinicians to estimate the timing of infection. IgM is the first antibody produced in a viral infection while IgG is produced later; a blood test that shows more IgM specific to the COVID-19 virus tells clinicians that the patient may have had an active infection a few days ago while an IgG-heavy result implies the patient is further out from an active infection (4).
Methods of Testing
There are many different methods to test for the presence of COVID-19 antigens or antibodies. Though slow and expensive, RT-PCR tests are currently widely used to confirm who is currently infected by COVID-19 thanks to the test’s high level of sensitivity and specificity (5). Other point-of-care tests designed for more immediate results (lateral flow immunoassays, ELISA assays) are not recommended for use outside of research according to the World Health Organization (WHO) (6).
RT-PCR Tests

The genetic information of the COVID-19 virus is contained in a substance called RNA. RNA makes up the separate components of the virus, similar to how DNA is present in all of our cells. Reverse transcriptase polymerase chain reaction (RT-PCRs) tests can inform us of viral presence in our cells by detecting the RNA that encodes the COVID-19 antigens.
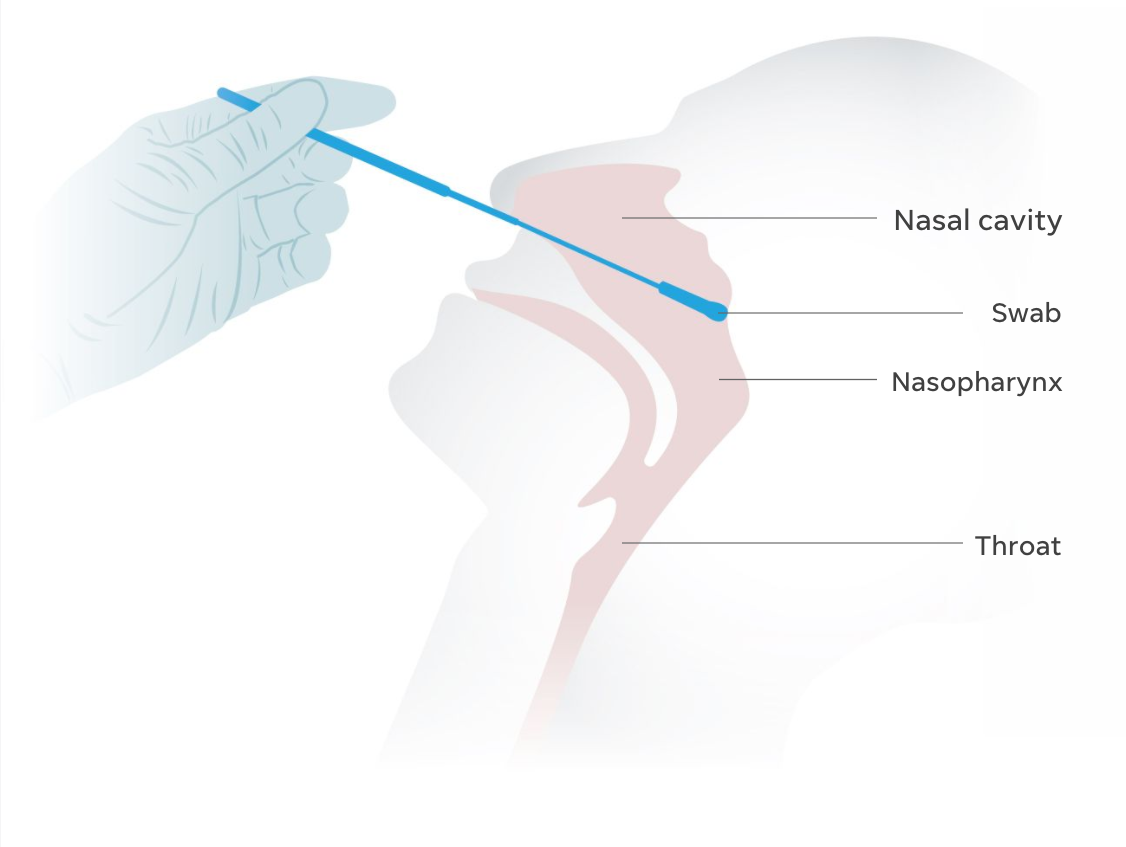
Samples are collected through a saliva sample (Figure 1) or through swabbing the nasal/back of the throat area (Figure 2). They are then sent to a laboratory to be analyzed for the presence of COVID-19.
Though this is the most reliable form of COVID-19 testing at the moment in terms of diagnosing patients, RT-PCR still has its drawbacks including risks of false-negative results (7). Because of this, many experts have called for the coupling of RT-PCR testing with CT scans in order to avoid inaccurate diagnoses (8).
Lateral Flow Immunoassays
The lateral flow immunoassay is a test that takes advantage of antigen-antibody binding to detect viral presence. A fluid sample is placed on one end of a nitrocellulose strip. Present on the strip are antibodies able to bind to the COVID-19 virus. As the fluid sample moves across the strip through capillary action, these antibodies will stick to any viral antigens in the fluid and travel with the fluid sample across the strip.

On the other end of the strip, the antibody-antigen particles will be collected and visualized, showing up as a line if the sample does have COVID-19 antigens (i.e. the patient is infected). There is also a “control line” to validate the strip is functioning properly (9). If this process sounds familiar, it is the same assay used for pregnancy tests! Figure 3 shows a diagram of this process.
This method of testing yields results very quickly and is often used as a Point-of-care (POC) test (10) - a screening test that is carried at the location of the patient themselves rather than in a separate laboratory, like RT-PCR tests (11).
Lateral flow immunoassays can also be modified to detect COVID-19 antibodies instead of COVID-19 antigens.
ELISA Assay
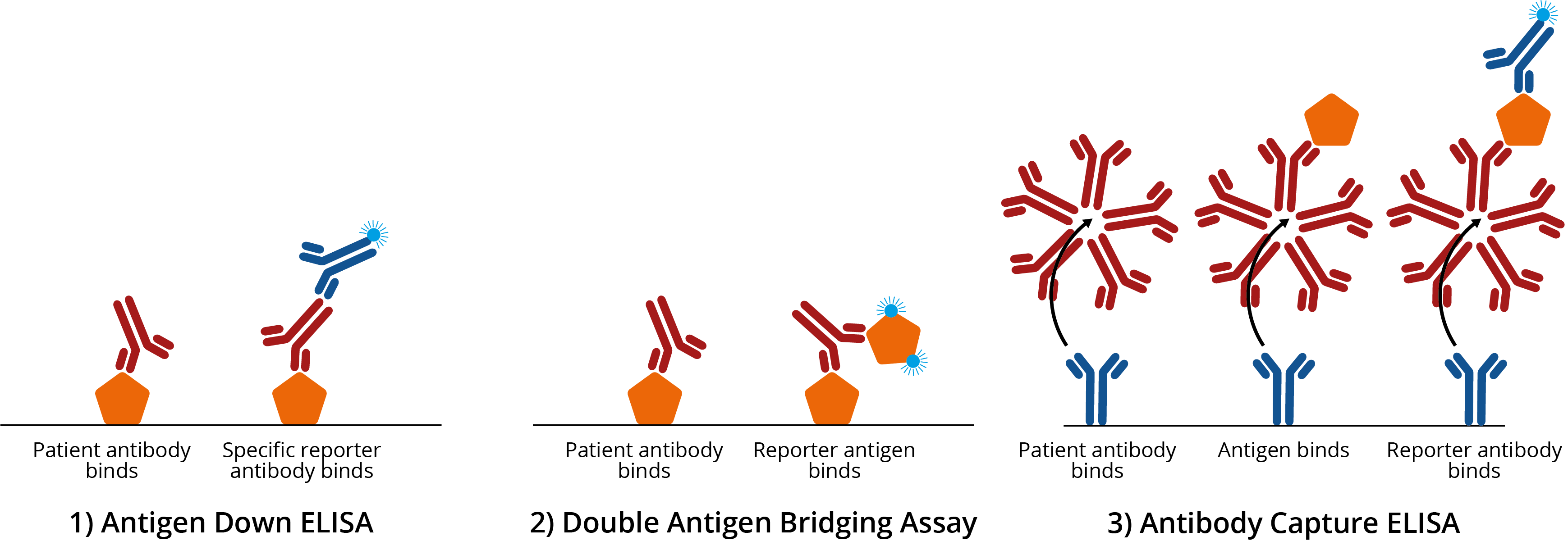
In an ELISA assay, a synthetic molecule that looks like a COVID-19 antigen is immobilized on a plate. A blood sample from the patient is then added to the plate. Finally, a fluorescent chemical called a reporter is added that lights up when it binds to human antibodies.
If the plate lights up, it is a sign that there are antibodies in the sample bound to the COVID-19 virus. The more the plates light up, the more COVID-19 antibodies are present in the sample (12). See Figure 4 for a diagram.
Screening Accuracy
The accuracy of COVID-19 tests has been difficult to determine because of their novelty. It is imperative to develop tests with high levels of accuracy in order to avoid misdiagnoses. There are two types of “wrong answers” that a failed COVID-19 test can yield:
False-positive results: healthy patients who take the test will receive a result saying they have COVID-19, leading them to mistakenly believe they are infected. False-positive results can arise if a test detects cross-reactive antibodies; these antibodies recognize a variety of pathogens/antigens in the body, not just COVID-19 antigens. A person who has never had COVID-19 but has these cross-reactive antibodies could then be labeled as infected.
False-negative result: infected patients are told that they do not have COVID-19. This is arguably the more concerning misdiagnosis because the infected patient may not receive the care they need and can unknowingly go on to spread the virus.
Accuracy of a COVID-19 test is typically measured along two metrics: sensitivity and specificity (13).
Sensitivity is how likely the test is able to detect the presence of COVID-19 in patients who are infected.
Specificity is the ability of the test to distinguish between those who are infected and those who are healthy.
Accuracy is affected by several factors (14):
The time at which the sample is collected matters. If the individual’s sample is collected too early on in the infection, the concentration of the virus may be too low to be detected. The same problem occurs when the sample is collected when the disease has progressed too far as well.
The sample may be contaminated when handled, leading to inaccurate results.
Samples that are stored too long (from extended transport or handling) can result in inaccurate results, particularly for RT-PCR tests since RNA samples tend to break down more easily.
Researchers at University of California San Francisco and University of California Berkeley have launched a study to investigate the specificity of COVID-19 antibody tests. For a dozen of these tests, the researchers have found that although they generally successfully detect COVID-19 after about 2 weeks of infection, many of the tests have high false-positive rates (15). Because of these troubling inconsistencies, the American Medical Association has warned against using the results of antibody tests as “immune certificates” or as excuses to discontinue social distancing behavior (16).
Though more reliable than antibody tests, RT-PCR tests are not perfect. The COVID-19 RT-PCR test called ID NOW (17) has been found to have a false-negative rate of about 15%. Another RT-PCR test called the Simplexa COVID-19 Direct (18) yielded a false-negative rate of about 10%. More accurate tests are being developed with lower false-negative rates (19).
How can I get tested?
The US Center for Disease Control (CDC) asks that you call your health provider if you show symptoms for COVID-19 and want to get tested. Your state's health department's website will also have specific information on testing guidelines in your state/area. Please note that it may still be difficult to find a testing center. The CDC has also released a guideline on how to interpret test results here - please use this to learn which course of action you should take following testing for COVID-19 (20).
Results from ongoing research and the current understanding of COVID-19 are constantly changing and growing. This post contains information that was last updated on May 18, 2020.